Free Shipping
on orders over $150.00
$0.00
$150.00
Add $150.00 more for free shipping!

TL;DR:
- Cannabis stigma is rooted in cultural, legal, and moral beliefs rather than scientific evidence, affecting access and disclosure. Despite increased legalization, social disapproval persists across many communities, driven by misinformation and deep-seated attitudes. Education and honest conversations are essential to reducing stigma and aligning public perception with research findings.
Cannabis stigma is defined as the social disapproval and negative stereotyping directed at cannabis users, rooted in cultural, legal, and moral beliefs rather than consistent scientific evidence. Understanding cannabis stigma matters because it shapes how people access care, disclose their use, and make decisions about their health. Public support for cannabis legalization rose from 31% in 2000 to 70% by 2023, yet social disapproval persists in workplaces, clinics, and families across Canada. That gap between legal acceptance and social acceptance is exactly what this article unpacks.
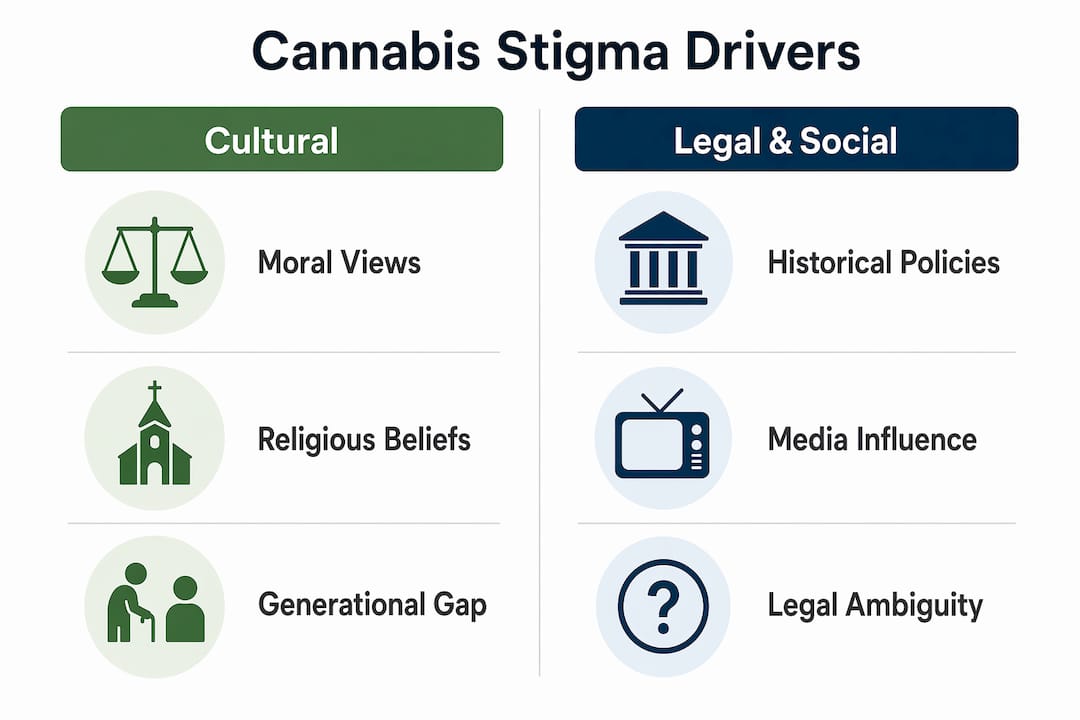
Cannabis stigma and society are deeply intertwined, shaped by decades of prohibition-era messaging, moral frameworks, and incomplete information. Three forces drive it most consistently: cultural norms, legal history, and misinformation.

Cultural and moral frameworks
Many societies have long framed cannabis use as a moral failing rather than a health behaviour. Religious traditions, conservative family values, and “war on drugs” rhetoric from the 1970s and 1980s all reinforced the idea that cannabis users are irresponsible or deviant. These attitudes do not disappear overnight simply because a law changes. Legal status does not guarantee social acceptance; users often face stigmatisation even in fully legalised contexts, particularly when others conflate recreational use with addiction or moral weakness.
Legal ambiguity and historical policy
Canada legalised recreational cannabis under the Cannabis Act in october 2018, yet legal ambiguity still fuels stigma. Many Canadians grew up under prohibition, and that conditioning runs deep. Workplaces, housing providers, and some healthcare institutions still treat cannabis use as a red flag. The blurred line between medical and recreational use adds another layer of confusion, making it harder for people to talk openly about why they use cannabis at all.
Misinformation and the information gap
Cannabis stigma persists partly because education has not kept pace with legalisation. Medical professionals often receive little training on cannabis, leaving patients without reliable guidance. Social media fills that void with anecdotal stories, which spread faster than peer-reviewed research. Younger adults tend to hold less stigmatising views, partly because familiarity with cannabis reduces stigma, especially among people under 35.
Pro Tip: If you want to understand why someone holds a stigmatising view, ask about their first exposure to cannabis information. Most people trace their beliefs back to a specific cultural moment, not scientific evidence.
The perception versus evidence gap is the single biggest driver of cannabis perception issues today. Public beliefs about cannabis safety and efficacy consistently outpace what clinical research actually confirms.
Social media algorithms amplify anecdotal cannabis success stories rather than nuanced clinical findings. A viral post about cannabis curing anxiety reaches millions; a carefully designed clinical trial with mixed results reaches thousands. That imbalance shapes what people believe before they ever speak to a doctor or read a credible source. The result is a public that is simultaneously over-optimistic about benefits and under-informed about risks.
One of the most persistent cannabis myths is that because cannabis is a plant, it is inherently safe. The “natural equals safe” fallacy leads people to downplay the real risks of high-THC products, which have become dramatically more potent over the past two decades. Modern concentrates can reach THC levels far above what research on therapeutic use was built around. Treating all cannabis as equivalent ignores a meaningful safety distinction.
| Public belief | What research shows |
|---|---|
| Cannabis is safe for everyone | Evidence supports use for specific conditions; risks vary by age, genetics, and frequency |
| Legalisation means medical endorsement | Legal status reflects policy, not clinical approval |
| Natural cannabis is safer than pharmaceuticals | Potency and delivery method significantly affect risk profiles |
| Cannabis is not addictive | Cannabis use disorder is a recognised clinical condition |
| More use equals more benefit | Dose-response relationships are complex and not linear |
Pro Tip: When evaluating a cannabis claim online, ask one question: is this based on a controlled study or a personal story? Both have value, but they answer different questions.
Closing the perception-evidence gap requires cannabis stigma education that is honest about both benefits and risks. Adults who understand the actual evidence are better equipped to make responsible choices and to push back on both over-criminalisation and over-promotion.
Cannabis stigma is not uniform. It shifts dramatically depending on geography, generation, and whether a person uses cannabis for medical or recreational purposes.
International survey data from 25 countries shows that moral opposition to cannabis is culturally relative. In countries with strict traditional social structures, such as Indonesia, over 90% of respondents labelled cannabis use as morally wrong. Canada sits at the more permissive end of the spectrum, but significant pockets of moral opposition remain, particularly in older and more religiously observant communities. Countries with strong public health education consistently show lower moral opposition, which points directly to the role of information in shaping attitudes.
For a broader look at how cultural attitudes shape cannabis views globally, the variation is striking even within regions that share similar legal frameworks.
Medical cannabis users face a specific and often overlooked form of stigma. They must navigate two competing judgements: the assumption that their condition is not serious enough to warrant cannabis, and the suspicion that they are using a diagnosis as cover for recreational use. This double bind discourages disclosure and can delay appropriate care.
| Group | Stigma level | Primary driver |
|---|---|---|
| Adults 55 and older | Higher | Prohibition-era conditioning |
| Adults 35–54 | Moderate | Mixed exposure to reform and older norms |
| Adults 18–34 | Lower | Greater familiarity and peer normalisation |
| Medical users (all ages) | Context-dependent | Blurred medical/recreational boundary |
| Rural Canadians | Higher | Cultural conservatism and less exposure |
The social stigma of cannabis is not a monolith. Recognising that it operates differently across groups is the first step toward addressing it effectively.
Overcoming cannabis myths requires more than legalisation. It demands education, honest communication, and a willingness to engage with evidence rather than assumptions.
Lead with education, not advocacy
Cannabis stigma education works best when it is grounded in facts rather than promotion. Adults who receive balanced information, including both therapeutic potential and real risks, are more likely to form nuanced views. Health Canada’s public education resources and peer-reviewed journals like Cannabis and Cannabinoid Research provide reliable starting points. Dispelling common cannabis myths is most effective when it addresses the specific misconceptions a person already holds, rather than delivering a generic pro-cannabis message.
Practical strategies for reducing stigma
The role of healthcare professionals
Changing cannabis stigma requires shifts in healthcare professional attitudes, not just public opinion. When a doctor dismisses a patient’s cannabis use without discussion, it reinforces shame and discourages honest disclosure. Training programmes that include cannabis pharmacology and patient communication skills are a direct investment in reducing stigma at the clinical level.
Pro Tip: The most persuasive conversations about cannabis happen one-on-one, not in comment sections. If you want to shift someone’s view, ask questions before making statements.
Cannabis stigma persists not because of evidence, but because cultural conditioning, legal history, and misinformation have consistently outpaced public education and honest dialogue.
| Point | Details |
|---|---|
| Stigma outlasts legalisation | Legal reform does not automatically produce social acceptance; attitudes shift more slowly than laws. |
| The perception-evidence gap is real | Public beliefs about cannabis safety consistently outpace what clinical research confirms. |
| Stigma varies by group and culture | Older adults, rural communities, and medical users face distinct and often compounding forms of stigma. |
| Disclosure affects care quality | Anticipated stigma causes patients to hide cannabis use from doctors, directly harming health outcomes. |
| Education is the most effective tool | Countries and communities with stronger public health education show measurably lower moral opposition to cannabis. |
I have watched the conversation around cannabis change dramatically since Canada legalised in 2018. The legal shift was real and significant. But what struck me most was how little it changed the social dynamics for many people I spoke with, particularly older adults and medical users.
The uncomfortable truth is that stigma lives in relationships, not legislation. A person can legally purchase cannabis at a licensed retailer and still feel they cannot mention it to their family doctor. That gap between what is permitted and what is socially safe is where the real work happens.
What I have found is that the most effective stigma reduction does not come from grand advocacy campaigns. It comes from individuals having honest, specific conversations with people they trust. A son explaining to his father why he uses cannabis for sleep. A patient asking their pharmacist about interactions. A colleague mentioning their prescription without apology. These moments accumulate.
The evidence also points somewhere uncomfortable for cannabis advocates: the perception-evidence gap runs in both directions. Some people overestimate harm; others underestimate it. Both distortions feed stigma in different ways. The path forward is not cheerleading for cannabis. It is a genuine commitment to evidence, even when the evidence is inconvenient.
If you are reading this because you use cannabis and feel judged for it, know that the stigma you experience is a social construct with a traceable history. It is not a verdict on your character. Understanding that distinction is the first step toward changing it.
— Juiced
Greensociety believes that informed adults make better decisions, and that starts with cutting through the noise around cannabis perception issues.
Whether you are new to cannabis or reassessing your choices after years of use, Greensociety’s educational resources give you the context to shop with confidence. The cannabis flower buying guide walks you through exactly what to look for when selecting products, from potency and strain type to sourcing and quality indicators. For adults who want to move past the myths and make grounded decisions, Greensociety’s blog covers everything from selecting cannabis flower online to understanding product categories across the full range of formats available in Canada.
Cannabis stigma is the social disapproval and negative stereotyping directed at people who use cannabis, rooted in cultural, legal, and moral beliefs rather than scientific evidence. It persists even in legalised contexts and affects how people disclose use, access care, and interact socially.
Legalisation reduces legal consequences but does not automatically reduce social stigma. Research confirms that users continue to experience stigmatisation after legalisation, particularly in healthcare and workplace settings.
Anticipated stigma significantly reduces disclosure to healthcare providers, which means doctors cannot account for cannabis use in treatment decisions. This directly affects care quality and patient safety.
Familiarity with cannabis use reduces stigmatising attitudes, especially in younger people. Adults under 35 are more likely to know someone who uses cannabis, which normalises the behaviour and reduces moral judgement.
Education grounded in balanced evidence is the most effective tool. Countries with strong public health education show measurably lower moral opposition to cannabis, confirming that informed populations stigmatise less.